August 2021
Wednesday 11th August 2021
Appointment with the oncologist, Dr. Goodman
The good news is that the results of all my tests show that chemotherapy is not advisable. Phew. What a relief!
In advance of this appointment, I had made the following list of questions and observations based on the referral letter from the surgeon to the oncologist. These are in black, and the replies and further observations are in red.
1. Was the tumour “invasive”? I was told it was at my first appointment with Mr. Memon. In his letter, he referred to it as LCIS (lobular carcinoma in situ). What difference does this make?
Both – two different types. Apparently all lobular carcinomas are “invasive” – but mine was also confined to the lobule.
2. Pleomorphic – rare, anomalous. Any significance relating to ongoing treatment?
Slightly increased risk of developing cancer in the other breast, but the radiotherapy and hormone therapy will reduce this risk.
3. Staging – Nurse at Breast Unit said they don’t usually take staging into account but I found this interesting: I have discovered that HER2 negative tumours of the size of mine (3.2 cm) which haven’t metastasised into lymph nodes or away from the breast, are classified as Stage 1B.
He looked it up and said that was probably about right, and then said that my tumour was actually Stage 2A, which means it was invasive, between 2-5 cm in size, and had not spread to the lymph nodes. My tumour was therefore T2, N0, M0 (stage 2 tumour – in breast only, early stage; no lymph node involvement, no metastases). (My colon cancer was T3, N1, M0, and Grade 4, the most aggressive with highly undifferentiated cells, which meant that chemo was required. My breast cancer is therefore less severe.) The Oncotype result trumps everything else, though.
4. NPI – Nottingham Prognostic Index. Score 3.64 = moderate:
5-year survival rate estimated at 90%
10-year survival rate estimated at 78%, by which time I will be 78 years old.
These look pretty good odds.
Are these statistics based on no chemo? From the letter, it would appear so.
He didn’t speak about this but said the Oncotype result was the most important.
5. Oncotype – what was result? Below 25?
I have discovered that for people over 50 with score below 25 would not benefit from chemo.
Result: 21. Chemotherapy is therefore not recommended. He gave me a copy of the Oncotype report.
6. Radiotherapy
(a) When do I start?
Either the week beginning 6th or 13th September.
(b) How many sessions?
Five.
(c) Daily?
Yes, Monday – Friday.
(d) What exactly happens?
With radiotherapy following lumpectomy, the risk of recurrence is less than 5%. Without radiotherapy, one-third of women have a recurrence. Radiotherapy will be to the whole breast, but not the lymph node area which was free of cancer. I will most likely have the “breath-hold technique” which means that for each burst of radiation, I will be instructed to take a deep breath and hold it for the duration of the radiation burst. This apparently allows the body to shield the heart (more vulnerable with treatment to the left breast) and the lung. There will be a planning session at the Oncology Department in the next two weeks, which will include a CT scan of my chest with breath-hold. (See note below about seeing the member of the planning team after my appointment.) 6-8 weeks after radiotherapy, I will have a review appointment, which will probably be by phone. Then, if all is well, I will be referred back to the Breast Unit for follow-up mammograms which will be on an annual basis.
(e) How long does each session take?
About 20 minutes.
(f) Any special preparations beforehand?
No, just the planning session, which will include marking with tattoos, which will consist of three dots (permanent).
(g) What side effects can I expect?
About 2 weeks after completing the treatment, I can expect to experience fatigue lasting 6-8 weeks. The best way to deal with it is to keep as active as possible. I said I already had underlying fatigue with my ME and he said I may not notice any difference. I can expect red, itchy and sore skin especially around the nipple, and in the fold under the breast, where there may be blistering. This should heal in about a week. It may need a gel dressing or natural oil moisturiser. The radiotherapy team with advise on management.
Longer term effects: the breast will become firmer and smaller over time. There will be some areas of tenderness around the treatment field and this should settle in a few months, but it may take several years. 10 years on, 1% of people have rib or lung problems after radiotherapy.
7. Hormone-blocking treatment
(a) When do I start?
Immediately. He gave me a prescription which had to be filled at the hospital pharmacy. He said he would be writing to the GP and after this first month’s worth of tablets, I would get the prescription from the GP as normal.
(b) What will this be?
(i) Oestrogen receptor blockers, e.g. Tamoxifen?
No – Tamoxifen carries a risk of blood clots and is contra-indicated in view of the fact that I am anticoagulated.
(ii) Aromatase inhibitor, e.g. Letrazole? Main treatment for post-menopausal women?
He said aromatase inhibitor therapy was better for lobular cancer than Tamoxifen. These drugs block the enzyme aromatase which produces oestrogen. He originally suggested anastrozole (Arimidex). I asked whether it contained lactose, and was told that it contains 68.75 mg lactose (quite a lot). I said that being vegan, I would prefer to avoid lactose, so he advised examestane (Aromasin) instead, another aromatase inhibitor, which contains no lactose. The third alternative, letrazole (Femara), also contains lactose, so if examestane doesn’t suit me, my options would be limited. I will be on this treatment for five years.
(c) I would prefer least systemic form of treatment, i.e. more targeted if possible. Reduced risk of side effects?
He said that both types of treatment were systemic, and that side effects were inevitable, but everyone is different and not everyone suffers severe side effects.
(d) What side effects can I expect?
Menopausal symptoms (e.g. hot flushes). Joint stiffness and pain, especially early morning or after prolonged inactivity, until I get moving. If this problem is severe, they would suggest trying a different drug (unfortunately both of which contain lactose). Examestane can cause osteoporosis, so they will conduct a bone density scan soon (a non-invasive, X-ray type examination) to check if my bones are already thinning. I will probably need some treatment to prevent this.
8. Phyto-oestrogens
Excellent treatment for menopausal symptoms – I took soy isoflavones and sage extract.
Have discovered benefits when on hormone blocking therapy for breast cancer – ARTICLE.
Whole-food plant-based lifestyle for approx. 2 years now, incl. soya. Interested in nutrition.
I showed him the list of links regarding various studies which indicate that phyto-oestrogen intake can be beneficial, and he said that for every study which suggested this, there was another study which contra-indicated it; the situation was confusing. A trial had been proposed which might have clarified things but this was cancelled when another study indicated that the use of hormone replacement therapy increased the risk of breast cancer (not the same thing, and I said it was a shame because it could have produced some useful results, and he agreed.) He said that it was probably inadvisable to take supplements (e.g. soy isoflavones with black cohosh, which I’d taken to great effect during the menopause) because it seemed counter-productive to be inhibiting oestrogen and then adding something else that mimicked it – I pointed out that one of the studies on the list showed that phyto-oestrogens acted differently and actually helped the activity of the aromatase inhibitors, but he stood his ground and said it wasn’t advisable. However, he said there was no evidence to suggest that removing all phyto-oestrogens from the diet had any beneficial effects, so I can go on eating my soya products. I have to accept that there are differing opinions on this subject, and conform to his advice. I am hoping that the side effects will be minimal, and we will just have to cross that bridge when the time comes.
8. Reasons for refusing chemo – Not now relevant. Only mentioned (a) and (b).
(a) Previous experience horrendous – never felt so ill. I said I was very glad to hear that chemotherapy was not advisable in my case, because my previous experience of it was horrendous and I have never felt so ill, and did not want to have to go through that again.
(b) Still experiencing effects from first time, six years on.
(c) Don’t want to lose my hair. Not relevant.
(d) With radiotherapy and hormone therapy, already covered by 2 adjuvant therapies.
(e) Risks associated with refusing? Not relevant.
After seeing Dr. Goodman, I saw Carrie, one of the planning team, who instructed me in the breathing technique known as “breath-hold” which causes the body to provide its own natural shielding of the heart and lung, and told me to practice it. She gave me an appointment for the CT, Planning and Mark-Up appointment (3 p.m. on Wednesday 18th August, a week today), and said I would be marked twice, once in resting position and the other while holding my breath, and the difference would be observed. With some people there isn’t much difference, in which case the breath-hold technique would be of little benefit, and they would provide some physical shielding to protect the underlying organs.
Later that day, I realised that the appointment she had given me co-incided with a funeral we were hoping to attend. I was able to contact the oncology department and change this to Friday 20th August at 1.30 p.m.
Thursday 12th August 2021
I had a phone call from the covid unit requesting that I make an appointment for a swab two days in advance of my appointment. I explained that we were due to be away that day attending a funeral. It is the same procedure I had to undergo before my operation – the swab two days in advance of the procedure in order to allow time for the result to be obtained, during which time both my hubby and I would be required to self-isolate. I explained the position to her that my hubby was in hospital and at this stage we didn’t know how long he would be in or whether he would require surgery. She was sympathetic and said she would contact the oncology department and appraise them of the situation. She was not aware that I had changed my appointment from the Wednesday to the Friday, and said that at least this gave us a couple of extra days’ grace.
She then suggested that it would be possible for me to have the swab the day before the procedure, as long as it wa done early enough in the day to allow time for the result to come through. At this stage I was unable to make any decision, not knowing what the situation would be with my hubby. She fully understood and told me to leave it with her.
Friday 13th August 2021
My hubby was discharged from hospital late afternoon, feeling very much better and not requiring an operation. On Wednesday, I had not had the chance to discuss anything with him regarding the oncology appointment and its outcome, because on our arrival home I immediately had to prepare a late lunch, and then he was feeling too unwell and had to arrange an appointment to see the GP, who immediately sent him to A&E so I didn’t see him after that. Once he was home again, I was able to go through everything that was said, and we discussed the difficulty of the covid swab and subsequent self-isolation, in association with attending the funeral. I told him I would be phoning the covid unit the following morning (Saturday) to request an early appointment on Thursday morning, so that we could attend the funeral, and self-isolate on Thursday and Friday morning only, up to the time of my appointment on Friday afternoon. This seems to be the best solution to the problem.
Thursday 19th August 2021
I had my covid swab this morning at about 9.15 a.m. – we arrived early, and they were able to do it straight away. This time it was a lot better than my previous experience because I was allowed to do it myself, and apart from some gagging with the throat part, there was no discomfort. She was happy for me not to thrust the swab right up to the back of my nose, which really helped. As before, she said they would only contact me if the result was positive. She wished me well for my appointment tomorrow and we were off.
Friday 20h August 2021
Today at 1.30 p.m. I was back in the Oncology Department for my radiotherapy planning appointment. I didn’t have long to wait, and was taken in to their CT scanner room. I undressed my top half and put on one of their clever little breast examination gowns which have various poppers so that they can expose just the bits they want.
The CT scanner platform had a different top on it from the usual – as the MRI scanner did for breast examinations. They obviously have a lof of different platforms that they can install according to the purpose of the scan. This time it looked pretty horrifying – all hard metal, and it looked extremely uncomfortable! Here are some pictures I found online.
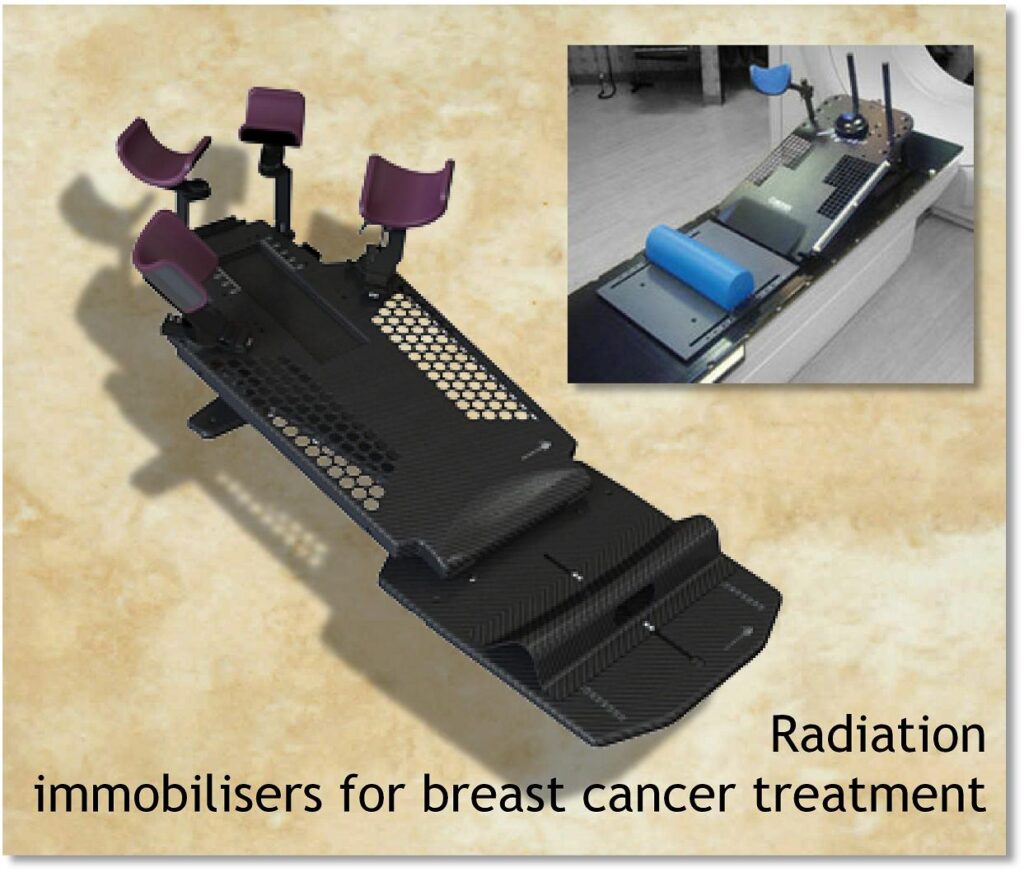
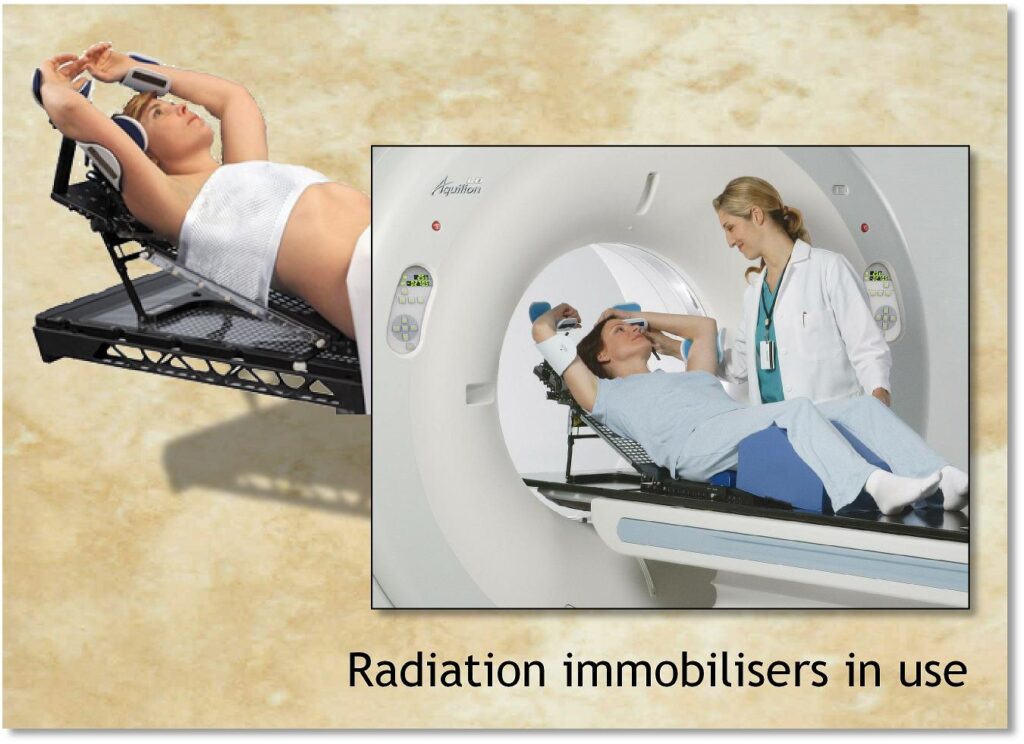
When I first saw it, I was instantly reminded of an episode from Star Trek The Next Generation (Schisms) in which the crew of the Starship Enterprise were abducted by aliens and experimented upon. This was their reconstruction of the the table they used.
All metal with strange projections!
I am always reminded of science fiction when I undergo any medical procudures…
It did indeed prove to be pretty uncomfortable, but they adjusted all the various positions and eventually it wasn’t too bad. Everything was adjustable, and marked with letters and numbers, so that they will be able to adjust the table I shall be on for the actual treatment in the identical position. Having my arms above my head like that for about 20 minutes did make my hands go to sleep but that is a discomfort I can put up with in the short term. I was instructed in the “breath-hold technique” designed to put distance between my breast and my heart and lung underneath which will be vulnerable to the radiation, and they said I performed brilliantly on the two practice runs, and then when they ran the CT scanner – I told them I was a singer and knew about breathing! When they asked if I’d be able to hold my breath for 20 seconds I told them that was a doddle – I could hold it for more than a minute. When they went into the other room and tested to make sure I could hear them when the scanner was on, one of them said “Choir practice begins in two minutes”! Haha! It really wasn’t a problem. Afterwards they said that all three breathing exercises were identical, and they were pleased.
Once they’d got me arranged as they wanted, they marked my breast with marker pens and did a lot of measuring, and then they added the tattoos. I told them I was disappointed to have been told previously that I couldn’t have a platypus tattoo – they were just dots! They laughed and said their artistic skills weren’t up to that level! I said they could make a fortune, setting up a tattoo parlour at the hospital. To make the tattoos they made an ink mark, and then pricked it with a needle, which was a little bit painful but it only lasted a second or two. I haven’t been able to look at them yet, as once the scan was done I got dressed straight away.
They do the CT scan to establish my internal anatomical arrangements as everybody is different in their proportions and measurements. Now they have all the measurements and the scan, they will put it all together and make a plan for my treatment. The radiologist will look at this plan and refine it if necessary. This procedure will take about two weeks, after which they will phone me with a definite date for my radiotherapy to begin. I asked if the sessions could be in the afternoons as that would suit me better, and explained that at the moment I am having to book my grocery deliveries a month ahead, and didn’t want to have to cancel them as I wouldn’t be able to move them to a different time. They said it wasn’t always possible to arrange this in advance, but one of them checked the list, and said I was definitely down for afternoon sessions (dates to be confirmed) so all is well on that score.
All in all this was a very interesting experience. A little uncomfortable at times but the fascination with what was going on, and the laughs and banter that took place between us all, more than made up for that.
Monday 23rd August 2021
I had a phone call today arranging an appointment for me to attend Paignton Hospital on Monday 20th September for a bone density scan (known as a DEXA scan). I have been waiting to hear about this, as Mr. Memon, my surgeon, told me that this would be necessary. I think it is a base-line test to check my bone density, because I am now taking the oestrogen blocking drug which could increase my risk of osteoporosis.
I asked what the test involved, and whether it would be invasive. She told me not – it is a low-level X-ray scan, so low-level that the radiographer is able to stay in the same room with me while it’s being done. I don’t know what part of my body they will scan yet, or whether they will scan the whole of me. It doesn’t sound as if it’s going to be much of a hassle.
I’ve looked it up online and got the information about how to read the results. I shall be interested to see if my bones are OK. I’ve never broken anything in my life. My hubby has broken 2 bones since we moved here in 2013! Perhaps he ought to be having the scan too!
I am already taking a vitamin D supplement, and eat plenty of calcium-rich vegan foods – I am pleased to discover that soya beans and their products are a rich source of calcium (see below, about phyto-oestrogens) and I’m eating loads of this now. Actually all legumes (beans, peas and lentils) are a good source of calcium. I’m also eating quite a lot of almonds. I have almond milk every day, and also make hummus from the pulp from making the almond milk.
Seeds are an excellent source of calcium, too, especially tahini (made by pureeing sesame seeds) – I eat a lot of this. Chia and flax seeds contain quite a bit of calcium too and I eat these on a daily basis. Always best to grind the flax seeds to make them available to the body.
Green veg is great too, but some are rich in oxilates which tend to inhibit the body’s uptake of their calcium, but boiling the veg does help reduce this. I eat quite a bit of spinach and kale which are low in oxilates. Fruit is good, especially oranges and dark red berries, of which I consume a great deal.
Our soya yoghurt from Tesco is also enriched with calcium, as is the tofu I am now consuming (see below for more on both of these).
It appears I have all the bases covered! Many people, in ignorance, think that if you live a dairy-free life, you are depriving yourself of much-needed calcium. However, it has been shown that consuming dairy raises the acidity of the body, which compensates by extracting calcium from the bones, in order to neutralise it – contrary to the belief that dairy, being rich in calcium, will feed and strengthen the bones. I think the statistics speak for themselves, actually – the highest incidence of osteoporosis is in Western nations which have a very high consumption of dairy products.
Natural, plant-based foods contain all the micronutrients that we need to sustain a healthy system (with the exception of Vitamin B12 which is recommended as a supplement for vegans). These micronutrients come packaged in a complex form with protein and fibre, and this orchestra of nutrients seem to work in concert with one another in a much more effective way than if you take them in supplement form. Nature is best!
Foods rich in vitamin D for vegans are fairly limited but spinach tops the list – I eat plenty of this! Also included are certain mushrooms, and foods which are fortified with it. In order to compensate for any dietary lack, I do take a vitamin D3 supplement.
I am hoping that my bone density will be at a healthy level, with all the good natural plant-based foods that I consume.
Effects of the exemestane
I’ve now been on exemestane, the aromatase inhibitor which blocks production of oestrogen, for about 10 days. I’ve had a few mild hot flushes, and some night sweats – I had terrible hot flushes during the menopause but never any night sweats. I’ve been adding soya to all my meals for the past few days in the hope of staving off the worst of the expected effects of a reduced oestrogen level in my body. I’m cooking up batches of soya beans and adding a tablespoon to my meals, including my oatmeal/chia breakfast! They are very neutral in flavour and it’s no hardship to have them. I’m also roasting cubed tofu marinated in various different ways – this is delicious. I am either eating them in my fingers or sprinkling them onto my food. I love the chewy texture which reminds me somewhat of chicken (which I no longer eat, being vegan). The tofu is also neutral in flavour and readily picks up the delicious flavours of the various marinades – I particularly favour spicy ones. This is all in addition to the soya milk that I regularly have (although I prefer almond milk in tea and coffee) and the delicious unsweetened soya yoghurt from Tesco that I eat with every meal! We get through loads of that.
I am so tanked up on phyto-oestrogens in my diet now that it should be enough to scare away any nasty menopausal symptoms – or at least reduce their severity.