Tuesday 5th May 2015
Oncology Appointment
I had my appointment with the oncologist today, 5 1/2 weeks after my surgery to remove the whole of my large bowel and rectum and create an ileostomy. I had been told that the surgery was considered curative, but would need some chemotherapy afterwards as “belt and braces” to mop up any rogue cells which might still remain in my system.
The histological examination revealed that my cancer was Stage 3 (invaded through all layers of the bowel wall, and also into one lymph node) and was Grade 4 (most aggressive) and the MDT were surprised when it was discovered because at my previous colonoscopy 18 months earlier, there had been no trace of it.
The oncologist is Dr. Lo, a charming Chinese lady who immediately put us at our ease. Also present was a visiting consultant from Germany, who very politely asked if I was happy with him being there, which I was. There was also a nurse present in the background, and later the specialist colo-rectal nurse arrived, and gave me the additional stoma bags I had requested on the phone in the morning.
I had been hoping for a single cycle of oral chemo but instead I was told that it would be intravenously over the next SIX MONTHS!!! I was horrified when she told us that. She said the oral stuff isn’t suitable for me because it can cause coronary artery spasm in healthy individuals and since I had one of those last summer, and also have left bundle branch block, it’s a no-no for me.
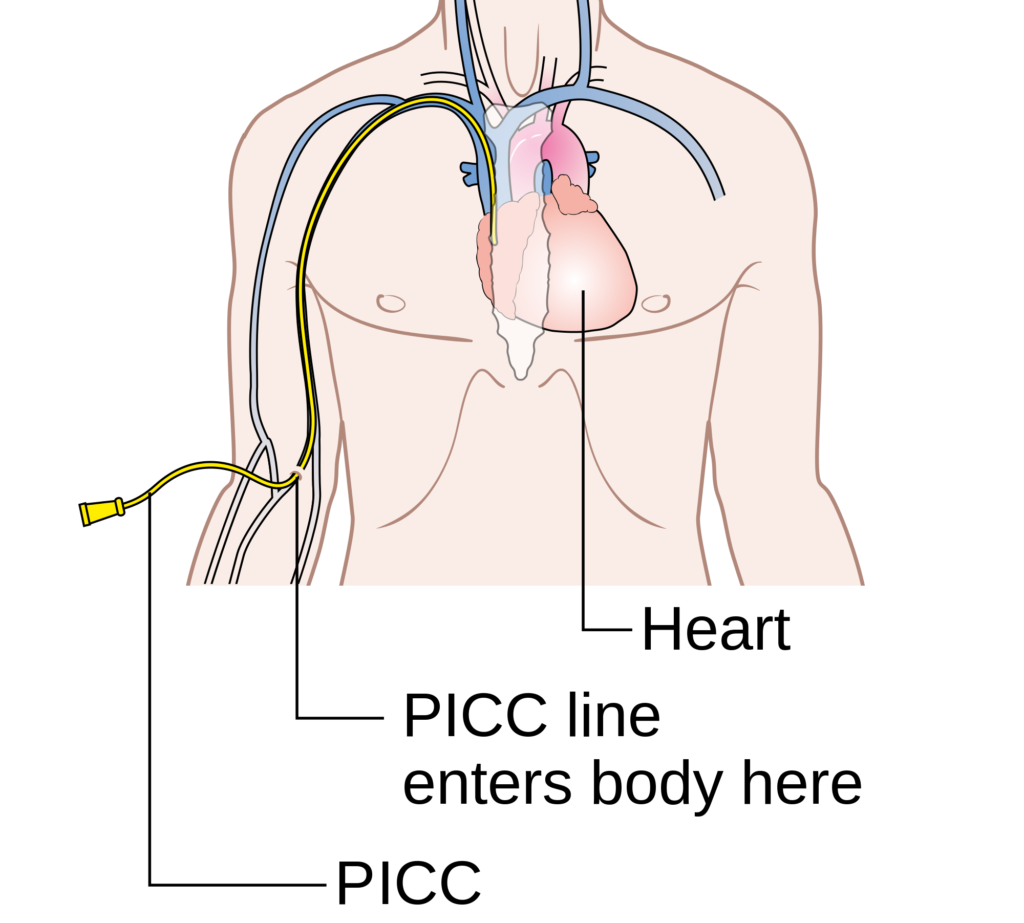
So I am having oxaliplatin (Eloxatin) intravenously, every three weeks, for six months. This is far more radical than I’d hoped, or even imagined would happen. She said I could have this via a cannula in my hand, and I baulked at this, given my horrendous experiences in the hospital when they were digging around for a vein and the pain reduced me to tears! She said the alternative was better anyway – I shall have a PICC line (peripherally inserted central catheter) installed for the duration of the treatment, and the chemo and any other drugs will be administered through the cannula in the crook of my elbow, from which they will also be able to take blood.
Also, I won’t get any pain in my arm that I might have got if they’d injected it through a cannula in my hand.
The PICC line will have to be flushed every week and I can have the district nurse to do that for me. The treatment will be administered by drip over about a four hour period. I’ve been warned about side effects which will be cumulative over the course of the treatment, and which will be most severe during week 1, then diminishing during week 2 until I feel more myself again in week 3 (“So lots of treats in week 3 then,” said my hubby).
Side effects obviously vary between individuals, but most people experience extreme fatigue. The drug reduces the number of cells in one’s blood. A reduction in the number of white blood cells increases the risk of infection; in red blood cells, causes anaemia. Reduction in platelets causes the blood to clot less readily, leading to bleeding and bruising.
The drug can cause peripheral neuropathy (numbness and tingling in the hands and feet). This is a common side effect, and it can be triggered by cold. Fortunately I am starting my chemo as the weather is getting warmer (well, it should be, anyway!) but it is recommended that one wraps up warmly, paying particular attention to the hands and feet, and the mouth and nose, because it can affect the mouth as well, and very cold drinks should be avoided. When taking things from the freezer it is recommended that you wear gloves.
Nausea should not be a problem because an anti-emetic is prescribed with the chemo, and also anti-diarrhoea medications are prescribed.
Some people develop some rather unpleasant side effects such as laryngeal spasm, causing difficulty with swallowing and breathing, or soreness in the mouth and mouth ulcers, and one’s sense of taste can alter, but these are less common side effects. Hair loss does not usually occur but some thinning may be experienced.
It all sounds pretty unpleasant.
I had no idea this was going to have to be so radical or so long-lasting. My friend Shaz has told me about the side effects etc., so I am not completely unprepared. Still, it’s put the kybosh on the whole of the rest of the year, which I hadn’t been expecting, but my hubby said, “Better that than a funeral service.” How right he is.
As we left, my hubby took me into the chapel, which is just near the oncology department. It’s absolutely beautiful. All around the altar are lots and lots of little teddies given in memory of babies who had died, and this moved me so much. Thinking of that made me count my blessings, and realise that whatever I’ve got to face, it’s never going to be as bad as that. The chapel is such a beautiful sanctuary and I’m so glad we went in there before coming home.
I will get a phone call in the next 5 days calling me in again, when they will talk to me about my treatment, and (I assume) fit the PICC line and do my initial blood test. Then they will tell me when the treatment will begin, which will probably be the following week. I didn’t think it would be so soon as I’d assumed they’d wait until after I’d seen the surgeon on 28th May, but Dr. Lo said they usually start it about 6 weeks after surgery, once things have healed and settled down.
I keep reminding myself that we should be grateful for this offer of chemo, however unpleasant it might be, because it’s only temporary and gives us the peace of mind we need. It’s just that it’s a lot more radical than I’d anticipated, and the whole thing takes a bit of getting used to. They’ve given me loads of paperwork to look at, including some excellent Macmillan books and leaflets. I must say, the whole MDT setup at the hospital is second to none, and however much people may moan about the NHS, I for one have had quite excellent treatment and care and I can’t fault them. I know I’m in good hands, and I’m confident of a good outcome.
I just hope I stay the course and can put up with it all… I am still finding it quite hard to get my head around the idea that I’ve had cancer at all, and haven’t been able to think about that aspect much until now, because my brain has compartmentalised it all, allowing me to focus first on the surgery, then on managing the stoma.
It’s a bit frustrating to think that I shall be made to feel poorly again just when I feel I am picking up after my operation and thinking I would soon get my life back again, but I feel it’s still on hold and will be for some time now.
Thursday 7th May 2015
More Bag Problems and Changing Body Shape
Over the past couple of days I started to get some itching again, and last night when we were out, it got so bad that I couldn’t wait to get home and take the bag off and see what was going on.
The skin was quite irritated again so obviously there had been some contact with output. I cleaned the area thoroughly and applied some Head & Shoulders shampoo which I left in contact for a few minutes (zinc content very good for skin problems) while I measured Kermit again – he now about 28 mm in diameter with a slight bulge – and cut a new bag to size. Once the H&S was rinsed off I prepped the area well with stoma powder and barrier wipe, and applied the new bag.
Within a short time – after I had put all the stuff away, of course! – I realised that there was a problem with this bag too, and pressing on the flange, realised that it did not seem to be sticking down properly, so I got everything out again and took it off.
This time I examined Kermit closely, and the surrounding area, and noticed that the “moat” which had developed recently and which had caused so many problems with leaks, had virtually disappeared. The stoma nurse had given me some Salts convex bags to help with this problem, and they were no longer working properly.
I decided to go back to one of my original Coloplast bags, with a Hollister ring, and also added a banana flange on the side nearest my tummy button, where there is still a crease in my abdomen where the first leaks occurred, and was pleased that for the rest of the evening everything seemed to be OK.
It is now mid-afternoon the following day, and so far so good! The itching has disappeared, and there don’t appear to be any leaks.
I shall be delighted if this situation lasts, because of the several bags I have tried, it is the Coloplast that I like the best. Fortunately I had several left when I was transferred to the convex ones, and when I see the stoma nurse tomorrow I shall discuss this with her.
The Hollister ring is rather thick, and I was a bit concerned that together with the bag flange, it came all the way up to the top of Kermit and I thought he might leak underneath again rather than outputting straight into the bag. Ideally what I would like is to use one of the new Trio silicone rings with the Coloplast bag – these are much thinner and automatically shrink to the size of the stoma, providing a good seal. I shall see what the nurse says tomorrow.
I am particularly pleased because the original Coloplast bags I was using are now available in the updated model which I like even better, with their very nice new covers, and I do hope I shall end up being able to use these permanently, and eventually get my home delivery set up, with these, the Trio rings, and also the Trio banana flanges which are brilliant – really thin, and transparent too.
I want to get this all sorted out before I start my radical chemotherapy which is due to begin perhaps next week. Once the side effects of the chemo kick in, I am sure the last thing I shall feel like doing is messing about with bag problems.
This is quite a rollercoaster ride, getting the right bag and accessories and a good fit – one minute I’m “up” and feeling we’ve finally got it right, and the next I am in the pit of despair and wondering if I’ll ever get this sorted! Eventually I know I will, and a year from now I shall probably be doing it in my sleep and looking back on this time with amazement. It’s just getting there that’s the problem!
The changes are due to my body settling down after surgery. The swelling from the operation is going down, Kermit is shrinking, and also my weight has been changing a bit. I lost about a stone (14 lb) in hospital, and then, when I came home, because my dear hubby will keep giving me delicious and tempting little pots of desperately fattening puddings, and the fact he needs continuous lessons in portion control lol – I gained about 7 lb! I also battle with the habit of “finishing everything on my plate” with which I was indoctrinated as a child – I hate waste! – if it’s on my plate, I will eat it!! Anyway, I am working on this, and so far have managed to lose a couple of pounds. I am not dieting as such; before the operation the surgeon had told me to hold off my diet until everything has settled down and I am better, because my body needs the nutrients for energy and healing; but I do want to eat as sensibly as possible and not undo all the good I did before. After he told me to stop the diet, and with the postponements in my surgery, I managed to gain 7 lb before going into hospital!
With all these changes to my body, the shape of my stomach is bound to be in a bit of a state of flux. The operation wound now forms quite a valley vertically down my belly, and I have noticed that I have developed a couple of “love handles” running diagonally downwards from my hip bones since the swelling has reduced – some internal bulk has been removed with the colectomy, and together with the weight loss, there is some sagging of my belly. Gravity, gravity, all is gravity… Maybe the NHS would be good enough to give me a tummy tuck if I tell them it’s for the benefit of Kermit? Hmm.. I don’t suppose they will! I thought it was jolly mean of the surgeon merely to laugh when I asked if he’d scrape out all my tummy fat while he was in there – all he said was, “No… I’m afraid everybody asks us to do that!” Shame.
Friday 8th May 2015
My First Blow-Out!
Shoshi has ARRIVED! She has had her first blow-out!
I had major problems this morning. I woke to find my first blow-out!!! It was very thick, fortunately, and hadn’t penetrated beyond my nightie, but it was on my right hand, and one very strange thing – I wear 2 silver rings, one on my thumb and one on the 2nd finger, and both these had gone a dark copper colour as a result of the reaction with Kermit’s output, but I’ve polished it off with silver cleaner and all is well again. When I was in Iceland all my silver jewellery went black from the sulphur fumes constantly in the air there from the volcanic activity, but this was a coppery brown with a few patches of blue-black which looked like blued steel. Interesting reaction between digestive enzymes and silver!
The top right of the bag as I look down had blown out and there was a great splodge of poo sticking out! When I got up and cleaned myself up, I noticed that the moat around Kermit had returned somewhat – it’s worse at the top when I’m standing, where my tummy is sagging a bit forward. So I’ve gone back with a Salts convex bag again. Thank goodness I’m seeing the stoma nurse this afternoon, so I’ll be able to discuss the problem with her. I’m also very glad that each time I’ve changed the type of bag I’m using, I have kept the remaining ones and not returned them to the clinic
It’s a real pain in these early days when everything is still shifting about and one’s shape keeps changing!! Sometimes I wish I was Tin Man and had a nice rigid stomach to stick the bag to.
I think part of the problem was that last evening my skin was itching, not immediately around Kermit (although of course the skin is quite irritated again this morning) but I’d put a banana flange on (Ostofix large frame from OstoMart) and I really don’t like them – they are hard to get off even with adhesive spray remover, and they do seem more itchy than the bag, and I had peeled it back a tad so I could have a good scratch, and the edge of the bag came up too – I pressed it all back firmly but the seal in that place may have been a bit compromised. Also, yesterday at lunch time my hubby made us a huuuuge cheese omelette (I keep on to him about portion sizes but he keeps giving me too much food, and I can’t get over the childhood injunction to “eat up everything on your plate” lol!) and I think the eggs may have bound me up a bit. The poo was quite thick (good thing, actually, or it would have spread much further) and it had pancaked a bit, and a lot of it was at the top of the bag, and the pressure probably caused the blow-out. So I’m not 100% convinced that the SenSura flat bag was the problem. I was lying down, of course, so it had no reason to flow to the bottom of the bag and keep Kermit clear.
One amazing thing – as I woke up I was vaguely aware of a slight poo smell and thought it was drifting along the landing from my hubby’s bathroom. There was barely any smell at all. I am now using a combination of a short spray of 3% hydrogen peroxide and a fresh mint tic-tac in the bag each time I empty, and it really does eliminate the odour!
I am hoping eventually to be able to have the Trio silicone banana flanges from my supplier – these are so fantastic. They have backing paper on both sides, and after you’ve applied the banana flange, you remove the top backing paper to reveal an ultra-thin, highly flexible and transparent flange which is practically invisible and which moves with your skin. Their silicone products are amazing.
A Good Stoma Clinic Appointment
This afternoon I had another scheduled appointment at the stoma clinic. I had spoken briefly on the phone last Tuesday with one of the specialist colo-rectal nurses about my problems with one of the HCAs and asked that I didn’t see her again, so I was a bit alarmed that she appeared to be on duty at the clinic today. I asked the receptionist who I was due to see, and he told me it was one of the CNS’s (Clinical Nurse Specialists) so I was relieved. The receptionist knew me by name, which was nice – but it does indicate just how much time I am spending in that place!!
While I was waiting, Dr. Johnston, the gastro-enterologist came through, and I had a nice chat with him, and while we were talking, my surgeon, Mr. Pullan, also turned up, wearing his scrubs! We all had a nice chat, and he said how well I was looking after my operation. I told them both about the six months of chemotherapy that I am facing and they both wished me well, and agreed that I have to look on it as a positive thing, making sure that all the cancer is gone for good. Nice to see my two favourite consultants!
My hubby was still parking the car when I was called in for my appointment. I was able to have a more detailed conversation with the nurse about the problems I had experienced with the HCA and she said she was sorry this had happened. I told her that I did not like to complain, but I felt it was important to let her know how things were, in case someone else was also affected, and I also had the opportunity to give her some specific examples. I repeated my request that I did not see that HCA again. I was glad my hubby was not there because this sort of thing makes him very uncomfortable (not that I enjoy it much either!) and he would much rather I left things alone and put up with it, but as I said to him, this is too important, and I need to have confidence in those who are caring for me, and sometimes things need dealing with, however unpleasant it might be at the time; in the long run, the benefits outweigh the temporary discomfiture. I feel very much better for having done it now, anyway, and the nurse was very understanding.
I then told her about the problems I’d had over the past few days. She took the bag off and said I still needed a convex bag. I told her how much I would like to go back to a flat one, because I so much liked the Coloplast SenSura Mio which is not yet available in the convex version, and she said that some people are able to use a flat bag again eventually, because after a period of time using the convex bag, the stoma gets pushed forward more, but it doesn’t happen with everybody. I said I didn’t mind, as long as I could have a decent convex bag, and I would certainly want to use the SenSura Mio convex if and when it was available.
She had another HCA helping her, who was also lovely and not at all like the other one! She made several trips to the cupboard for supplies for me, and the first convex bag they produced (can’t remember the name) I rejected almost at once, because the tail was horrible and it was a fiddle to undo, and like the OakMed one, it only had one rigid plastic strip so I could see myself getting output all over my hands again. The nurse suggested the Coloplast SenSura Convex Light bag – this is the convex version of my original bag, and I jumped at that one.
The tail is identical, and I really like this. It has the two rigid plastic strips, and when you press their edges together, the bag springs open beautifully, and I like the Velcro fastening wings too. This bag has a good viewing window, with the outer cover being divided so that you can lift it, and the top half of the bag under the cover is transparent. This is better than the Salts bag which was only transparent over the stoma itself. Another thing I like about the SenSura bags (flat and convex) is the fact that the edge of the flange is transparent, so you can see if a leak is advancing towards the edge, and deal with it in time.
The convexity is softer, and less pronounced than on my previous bags, and this is a good compromise between the rather hard and rigid deeper convex flanges and the flat bag.
One slight disadvantage is the paucity of measuring rings on the flange, which makes cutting it to size a bit more difficult, but the nurse gave me the backing sheet from the bag she put on me, to use as a template. She cut the hole circular, not worrying about the slight bulge on one side of Kermit, and said that it shouldn’t be too tight a fit, or the stoma might develop granulomas (small nodules which form as a result of friction from the bag) and these can bleed a lot. She cut the bag to around 28 mm.
I told her I was running out of some of my supplies, so in addition to supplying me with plenty of the new bags, she gave me a new pack of Conti wipes (these are the dry wipes that you can use either dry, or with water, and they are larger than a lot of the wipes supplied by the manufacturers of stoma care products, and you can cut them in half and get double the amount!), and plenty of barrier wipes (which the previous HCA had considered unnecessary!!).
I haven’t tried these Pelican barrier wipes, but my first adhesive remover spray was by Pelican and I liked that very much.
Finally, she gave me some more banana flanges to replace the few OstoMart ones I had left. I said I didn’t like those much because they made my skin itch (there are some small red spots where they had been) and she said she didn’t like them much either – a lot of patients had experienced skin irritation from them because they are far too sticky (even with adhesive remover spray they are very hard to remove) and do not allow the skin to breathe. She produced some by Salts instead.
These are thinner and more flexible, and although they look rather opaque when you first apply them, with the warmth of your body they become more transparent and adhere better than initially. They contain aloe vera and are a lot more skin-friendly than the OstoMart ones. Eventually I would like to get the Trio silicone ones through my supplier because these are a dream to use, but the nurse said they don’t deal much with Trio, because they only do accessories and the GPs are apparently pressing them to cut down on prescribing too many accessories. (The other HCA was just dismissive of Trio products and said, “We can’t stock everything…” and “I saw them at a trade fair and wasn’t impressed…”)
These banana flanges have backing papers on both sides. You remove the first one and apply the banana flange as normal, and then remove the top backing sheet, exposing a wafer-thin transparent strip which flexes with your skin and is breathable. I love these!
When the nurse removed my bag, she used plenty of adhesive remover spray without my having to ask her, and she peeled it off slowly and gradually, and I felt quite relaxed about it. She had no problem using barrier wipes either, but said the powder should only be used if the skin irritation was so bad that the surface of the skin was broken and moist, because otherwise the powder would not stick.
She said that we should now be thinking about getting a prescription set up for me, so that I can start receiving supplies via a home delivery service. I quite agreed, but said that things were still constantly changing, which was getting pretty boring! She said there was no point in setting up a prescription if the next week it had to be changed again! She has made another appointment to come in three weeks’ time, which will be on the same day as my follow-up appointment with Mr. Pullan, my surgeon, and hopefully by then, things will finally have settled down.
She warned me that the chemotherapy might affect the stoma – not necessarily its size or shape, but quite likely the output, which can increase in quantity and become much more liquid. She said I may need loperamide (Immodium) to help with this, but I said if I could correct the problem with jelly babies, that was preferable! (How I wish jelly babies were available on prescription!!) For the moment, the output is quite thick, which she was pleased to hear – although I did say I thought my blow-out this morning was partly due to pancaking because it was so thick!
As we left, both the nurse and the HCA were very sweet, and the HCA said, “Nice to see you again.” I said to my hubby on the way down, “What a great appointment! That’s how it is supposed to be!” I certainly didn’t feel like that on the previous two occasions! Coming out this time, I felt I had had a very positive experience, my questions and observations had been listened to carefully and responded to in a considered way; the atmosphere was friendly, and there was decent dialogue. Should we expect anything less?
Wednesday 13th May 2015
Plans for Chemo
When we were out Monday there was a message for me to phone the hospital regarding my pre-chemo “chat” appointment. I got through yesterday morning to the oncology day centre, and they told me a letter would be in the post, but I was to come in next Monday morning, and at the end of that appointment, my PICC line would be installed. The chemo would then begin the following day. I said that I had had second thoughts about the PICC line, having had the opinions of various other people, and also having done my own research; I said I would prefer to have a port-a-cath instead. She said she could not discuss medical matters, but would ask the specialist chemotherapy nurse to phone me about it.
I eventually managed to speak to her this afternoon, and said that in view of the fact that this treatment wasn’t going to be over in a few short weeks, but would be going on for six months, I would prefer to have the port-a-cath which is embedded in the chest with nothing to show. There would be less risk of infection (especially as one’s immune system is compromised by the treatment anyway) and I was concerned about the catheter remaining in my arm for so long, with the tails exposed and coiled up under a dressing when not in use, particularly with the onset of the summer weather.
She said that in principle there were no objections to my choice, but she would have to consult Dr. Lo, the oncologist, for her opinion, after which she would phone back to let me know.
It is more complicated to install than the PICC line, and is not a nurse-directed procedure but would require a radiologist. This doctor does two of these per week, on a Friday, and they would have to see when his next available slot came up. If this goes ahead, I would have to attend the hospital first thing in the morning to have the procedure, and then the chemo would start straight away. This would mean one less visit to the hospital, but I would be in all day.
The port-a-cath is a port, a small implantable device which is inserted under the skin of the chest, with a silicone rubber membrane through which a needle can be inserted for the administration of medication and the withdrawal of blood. Attached to the port is a catheter which leads into the subclavian vein on the right-hand side of the chest, and then into the superior vena cava, the main vein leading into the heart. Introducing chemotherapy into the body in this way is preferable to the use of peripheral veins because of the toxicity of the drug which can cause damage to the more delicate tissue of the smaller vessels.


Obviously this is a more complicated procedure than the insertion of the PICC line, but it will make life a lot easier and more comfortable in the long run, and the port-a-cath requires less maintenance too, so I am hoping that Dr. Lo will raise no objections.
My appointment on Monday is going ahead as scheduled anyway, and I shall know in a day or two which delivery method I shall have for the chemotherapy.
Thursday 14th May 2015
Provisional Update on Appointments
The specialist chemotherapy nurse phoned me again this morning to say that Dr. Lo approves of my choice to have the port-a-cath instead of the PICC line, and it now remains to fix an appointment with the radiologist to have it installed.
He performs these procedures on Fridays, and provisionally I am booked for Friday 22nd May, but failing that, it will be the following Friday, 29th May (the day before my birthday…). Immediately after its installation I shall begin my chemo.
I need to turn up really early (8.30 a.m. – eek! That’s the middle of the night for Shoshi!) but I probably won’t be allowed any breakfast because I’ll need a sedative, so I’ll get a bit more time to sleep before I have to get up.
Before the procedure, they want me to have a pre-assessment appointment (like before my bowel surgery), and it is possible that I will have this as part of my pre-chemo “chat” appointment on Monday; if this doesn’t happen, she will try and schedule it for Thurs. 28th if the procedure is being delayed till the 29th, because we will be at the hospital anyway on that day, for my next stoma clinic appointment and also the follow-up appointment with Mr. Pullan, my surgeon.
I am very glad they have agreed to let me have this procedure. OK, it involves more hospital appointments and will be a more complicated procedure for me to have to undergo, necessitating sedation, but I think in the long run that will be a smaller price to pay than dealing with the inconvenience of the PICC for such a long time. It should require minimal maintenance, and nothing will show on the outside except for a small bump.
Updates when I get them.
New Froothie Optimum 9400 High Speed Blender
My wonderful new blender arrived this morning! Having done extensive research over the past few weeks on whether I really needed/wanted such a machine (the answer was yes!) and then which machine to purchase, I finally made the decision, and went ahead and ordered it.
I had originally been drawn to the NutriBullet but various reviews online suggested that it didn’t do such a good job at getting things completely smooth, and it really wasn’t as sturdily constructed as the more expensive machines, and also was rather small. I’d rather put off thinking about the VitaMix which everybody has been raving about, on grounds of the cost, but it really is a superb machine and would answer my needs.
While looking at different reviews of this one, I came across one entitled “Don’t buy this blender” on Google, so I hopped over for a look and found myself on the Froothie site, looking at the Optimum 9400, which superficially looks very similar, but which is faster, more powerful and best of all, cheaper! I decided this was the machine for me, and if you explore the site you can see just how impressive it is – it will even crush rocks!!! (Not sure which is more stoma-friendly, though – granite or limestone…)
Since hearing that I needed an ileostomy, I was grieving for all my favourite foods that would no longer be available to me because of their fibrous nature and because they would be likely to cause blockages: fresh pineapple and mango, coconut, nuts, seeds etc. Even though I may no longer be able to enjoy their lovely textures, I can at least enjoy the flavours I have been missing. [Later – I am now able to eat all these things, with the caveat that everything needs to be well chewed.]
Of course, a blender like this does not remove the fibre; it merely pulverises it, so I shall have to be careful, especially initially, not to overdo the fibre intake or it might cause a blockage. I’m going to take it slowly, and my first smoothies will be small in size, and sipped slowly!
I will be able to make smoothies, nut milks and butters, soups, and all sorts of good things. The machine comes with a nice little recipe book full of healthy dishes, and of course there are masses of recipes online.
Now all I have to do is collect together some suitable ingredients and get started!
Monday 18th May 2015
New Patient Talk
Today I attended the hospital for my “New Patient Talk” in the chemotherapy department. This is set up so that the specialist nurse (in my case Catherine) can talk you through what to expect, and to answer any questions. They give you plenty of time, and also provide you with a “Patient Held Record” which is a small plastic-covered book with all the details of your treatment, appointments, medications, contact numbers, side effects and what to do about them, etc.
First of all, she told us that the chemo would start this Friday (22nd May) after the installation of the port-a-cath. I have to turn up at 8 a.m. (even earlier than I’d thought!) and will have to have an anaesthetic for this procedure, which means no breakfast. By the time this is all done, I shall begin my first chemotherapy infusion at 12.30 p.m., and it will take four hours, so it’s going to be a long day at the hospital.
Before this happens, I have to have a pre-assessment appointment with Dr. Isaacs, the radiologist. He will assess my fitness for the anaesthetic (as happened before my bowel surgery) so that they are aware of any potential problems and be prepared to deal with them should they arise. This appointment is on Wednesday 20th May at 2 p.m., so we will have had three visits to the hospital this week! (Next week I’ve also got a stoma clinic appointment, and my follow-up appointment with the surgeon on Thursday.)
The chemotherapy sessions will take place every three weeks and will last four hours. The infusion will be introduced into my body via a small needle assembly straight into the port in my chest, through which they will also be able to take blood.
Blood needs to be taken regularly because the drug affects the production of blood cells by the bone marrow, and they need to keep an eye on the levels of red and white blood cells (particularly neutrophyls), and platelets. I could become anaemic, and my immune system will be compromised, and also I will be susceptible to bruising, and possibly nosebleeds and bleeding gums because low platelet levels will affect the normal clotting ability of my blood.
Forty-eight hours before each treatment I shall have blood taken by my local surgery. We are going to arrange for the district nurse to come and do this for me, and the chemotherapy department will give us a form to drop in to the surgery.
The drugs I shall be given are as follows. The chemotherapy itself is oxalyplatin (Eloxatin), and I shall also be given ondansetron (Zotran) and domperidrone (Motilium), both of which are anti-emetics (to prevent nausea and vomiting) – these will be in tablet form, the former to be taken one every twelve hours, 48 hours after treatment and the latter if required, one tablet three times a day.
I may also be given a steroid tablet for symptoms of nausea as well but hopefully this will not be needed as steroids to tend to pile the weight on!
The period when my immune system will be most compromised will be between days 5 and 15 in the three-week cycle, and it is very important that I avoid contact with any source of infection, for instance crowds where there might be colds. Minor occurrences which do not affect one in the normal course of events, such as cat scratches and other minor abrasions, and the consumption of dairy foods made from unpasteurised milk (e.g. brie – that’s a shame – I love the stuff!) and yoghurt containing live bacteria (again, I’m disappointed, because I was hoping to continue enjoying my Fage Total Greek yoghurt!), can quickly lead to major infections which can be serious, if not fatal, if not dealt with promptly. I’ve also been told to avoid honey (another shame – I love honey, and also use it for sweetening things) because there’s apparently a potential risk of botulism, and pasteurising honey does absolutely nothing to destroy any possible Clostridium botulinum spores, which pass through the gut of a normal, uncompromised system without harm.
I have been given some telephone numbers in case I should start to feel ill with flu-like symptoms (aching joints and muscles, headache, feeling generally unwell and feverish), and somebody will be available to take my call 24 hours a day. At the first sign of any such symptoms, I am to take my temperature, and to phone the hospital if it is raised about 37.5 deg. C. It is important not to take paracetamol because this merely masks the problem by lowering the temperature and reducing the symptoms, but the infection would still be there and it could be extremely serious. If the hospital think it is necessary for me to go in, they will prepare A&E for my arrival, and the policy of the hospital is for the problem to be dealt with within one hour of being called in, which shows how seriously they take this potential problem.
This is all pretty scary stuff…
Because the chemotherapy works by attacking fast-dividing cells, it not only attacks cancer cells but also other, normal cells in the body such as blood-producing cells in the bone marrow, and the cells inside one’s mouth. This can result in a sore mouth and possibly mouth ulcers. I have been provided with two different mouth washes to use. The first is Chlorhexidine gluconate, which I should use as part of my normal oral hygiene – the nurse suggested I clean my teeth three times a day, using a soft toothbrush, and to use the mouthwash after this.

Should I develop ulcers, she gave me another mouthwash to deal with the problem: Difflam Oral Rinse (Benzydamine hydrochloride).

Another very common side effect is peripheral neuropathy – numbness and tingling in the hands and feet, and this can also affect the mouth. The symptoms are triggered by contact with cold, so it is important to wear gloves when handling food from the fridge, for example. Drinking chilled drinks and eating ice cream can cause symptoms in the mouth, and moving from a warm environment into the fresh air can also trigger symptoms, notably trachaeal spasm which can be alarming as one becomes temporarily unable to breathe. The nurse recommended bringing a scarf to my treatments, to cover my nose and mouth when leaving the hospital, and going from the car to the house.
The hands and feet can become sore, and the skin very dry and even cracked if not looked after, so she recommended keeping them well moisturised. I was very amused when she produced a pot of cream with a cow-hide design on it, called “Udderly Smooth” – she said that it had originally been designed for the udders of cows, but farmers found that it was great for their skin too, so it is now used as a human skin moisturiser! As long as this whole experience doesn’t transform me into a cow, I shan’t mind!

I must also expect to feel extremely fatigued and somewhat hung-over, especially in the immediate aftermath of each treatment, and I will need to rest a lot – but then, I am used to that.
The nurse went on to discuss the psychological effects of all this, and said how normal it was to feel afraid and anxious. There is plenty of support available to help, and there is a psychologist on the staff to help should I need to learn coping strategies, but I think this is unlikely – I am a strong person and have made sure that I am as well-informed as possible (fear of the unknown is probably the worst), and my faith in Jesus has carried me through thus far and I don’t anticipate Him letting me down at this stage! I am so grateful for everybody literally around the world who continue to pray for me, and I feel carried along by a tide of answered prayer.
There is a separate building on the hospital campus called “The Lodge” for cancer support, and there is always someone there to talk to; they offer massages and other pamperings, and counselling and just a place to chat with fellow-patients, etc. They have a drop-in centre several days a week, or you can make scheduled appointments.
Talking of cows, when we arrived, we sat in the waiting area to the side of a wide corridor, from which led a couple of wide doorways into the treatment area. There were lots of recliner chairs in there, occupied by people connected to IV poles, and beside each one was another chair for use by relatives etc. It reminded me of a milking parlour – all the people patiently sitting while the machines did their stuff (OK, stuff was going in, not coming out – you can stretch analogies too far!) and I did think it was somewhat lacking in privacy! I had expected to be in a normal ward, on a bed, or perhaps in a treatment room. Every now and again someone would get up and walk to the loo, pushing their IV pole, and I thought to myself that that would be fun, using a wheelchair! I’d have to have someone to help me! The whole setup was a very strange spectacle, and made all the more so by the thought that in a few days’ time, I would be joining their ranks. The nurse said how important it was to drink plenty of fluids; tea and coffee facilities are laid on, and they provide lunch as well.
Over the next six months I am going to become very familiar with the chemotherapy day unit; the nurse said that since most chemotherapy is given on a three-weekly basis, I shall probably end up meeting the same people each time. She said it is scary to start with, but one soon becomes very accustomed to the routine, until sometimes patients actually remind the staff about things and correct them if they make any mistakes!!
We have come home armed with masses of information and stuff to use, and it’s all fairly overwhelming…
Wednesday 20th May 2015
Pre-Assessment Appointment for Port-a-Cath
Today I had the pre-assessment appointment in advance of the insertion of the port-a-cath on Friday. This device will allow the injection of chemotherapy and other drugs and also the extraction of blood. It will be inserted under a light general anaesthetic with local anaesthetic being administered to the incision sites, and the procedure should take around an hour to complete.
This is more hassle than the insertion of a PICC line but in the long run it is going to be a lot less hassle to manage during the course of my treatment, so I think it is worth it. I was pleased that they agreed to my choice to have this done.
The device will be embedded in my chest with nothing to show on the outside except a small lump.
The specialist radiology nurse did the bulk of the interview, and it was a very thorough checklist indeed – more thorough than the pre-assessment before my operation, actually. She covered every area of my health, and said she would like me to have a blood test for INR (International Normalised Ratio – a determination of prothrombin levels which indicates the clotting properties of the blood) and also an ECG, for which she gave us the forms and told us to attend the heart and lung unit at the end of the appointment – you just hand in the forms and wait your turn.
She also gave me details of fasting prior to the procedure, and where to turn up at 8 a.m. on Friday – at the Ricky Grant Day Unit where the chemotherapy takes place, and after the admission process, I will be taken down to theatre for the port-a-cath to be inserted. She said she would be present during the procedure.
By the time she had finished, it was lunch time, and she said we had time to get ourselves something to eat before returning to see Dr. Isaacs, the radiologist, for the final part of the appointment. He went into more detail about the exact nature of the procedure.
He will make a small incision (approx. 5 mm) at the base of my neck on the right hand side after the administration of local anaesthetic, and under ultrasound guidance, access will be gained to the internal jugular vein.
Another, larger incision will be made below this, on the right side of the chest, about 3 cm long, also with local anaesthetic, and a pocket formed, into which the port will be inserted against the chest wall.
The catheter is fed through the small incision until it ultimately reaches the superior vena cava, the main vein leading into the right atrium of the heart, and then a small tunnel is made under the skin, for the other end of the catheter to be attached to the port. The correct positioning is determined by means of X-ray, which is why this procedure is carried out by a radiologist.
The two incisions are closed with dissolvable sutures and covered with a small dressing.
Dr. Isaacs said that as I was having my first chemotherapy infusion at 12.30 p.m., he would insert the needle assembly so that it was ready, to save them doing this just before the treatment begins.
I will be sent back to the Ricky Grant Unit to recover, and then my treatment will begin at 12.30 p.m. It will take four hours, and they will keep me there for a further half an hour just to make sure I don’t have any sort of reaction, before I will be allowed to go home. A long day at the hospital!
Dr. Isaacs had a port-a-cath with him, which he showed us. It is quite a small device (about 1/2 in across and about 1/4 in thick) attached to a long, thin, flexible line marked off in centimetres. The top surface is covered with a transparent silicone rubber membrane through which a needle can be injected many times without damaging it, and which “heals” after the needle is removed. This membrane felt a lot tougher and harder than I’d anticipated – having made silicone rubber moulds I had thought it might feel quite soft and thin, but it has to withstand quite a lot, and needs to be secure. Blood can also be extracted through this membrane.
Compared with the PICC line, it is maintenance-free between treatments. The PICC would have required weekly flushing with heparinised saline (Hepsal) (to prevent blood clotting in the line) but with the port-a-cath, this need only be done at the time of each treatment. With nothing to show on the outside but a small lump after the incisions have healed, it can be treated normally and doesn’t need to be kept dry – showering and other normal activities can take place in the usual way.
I will have had three hospital appointments this week! Then two more next week, but at least they are on the same day! There is now a well-worn path between home and hospital and I am beginning to wonder whether to take a sleeping bag and find a corner in which to doss down. This would save on petrol and all the hassle of parking each time.
Two days of wellness remaining till it all begins. I’m feeling so much better after my operation and keen to pick up the threads of my life again and now I shall have to put up with feeling poorly once more, but it’s all in a good cause!
Friday 22nd May 2015
Installation of Port-a-cath and First Chemotherapy Cycle
We arrived at the Ricky Grant Day Unit at 8 a.m. as arranged, and I was booked in for my procedure, with the usual lengthy form filling and Q&A sessions. I was given a hospital gown and told to strip my top half only, and put this gown on with the opening down the front. Very fetching. Then I went down to theatre on a trolley. There is a special theatre devoted to interventional radiology, where a radiologist performs minimally-invasive surgical procedures under X-ray guidance, accompanied by the usual anaesthetist and theatre staff. I was wheeled into the small anteroom which acted as an airlock and again was reminded of space travel – when I had my CT scan I imagined I was going through the stargate as per the TV series – the devices looked so similar! In this case, I was certainly going into outer space, or at least, being spaced out. They gave me a paper hat to wear, and then they went through the forms and Q&A again, and when I got into the theatre proper, they asked a lot of the same questions again, which amused me greatly – did they think that I would somehow be substituted for another patient during my passage through the door? Lol! I am not complaining – it is very reassuring that they are so thorough. Gone are the days that they cut off the wrong leg, or worse, the leg off the wrong patient!!!
While still in the airlock I was surprised when they ran through the checklist and said “two port-a-caths…” I said, “Two?” They said one was a back-up, in case they dropped one! It was a lot easier to start with two unopened packs, rather than having to search the hospital for another one if they had a mishap. I thought they could always drop me, if they dropped it, and then everything would be fine.
The theatre itself was amazing, with huge X-ray machines suspended from the ceiling and what looked like a vast wide-screen TV. (Shame I was going to be asleep for the duration and would miss all my favourite programmes.) One of the staff said not to worry – they knew it all looked rather intimidating, but I said not at all, I was fascinated.
They slid me onto the operating table and prepped me for surgery. Dr. Isaacs, the radiologist, carried out a brief ultrasound scan on my neck to locate the correct veins and expressed himself satisfied that I had “lovely veins” – how reassuring to know that!! This would show him where to make the first incision to insert the catheter. They placed an oxygen mask over my face. The insertion of the cannula into my left hand was again an extremely painful experience, as it had been when I was an inpatient, causing me to cry out for the whole duration of the procedure. After it was done, they said they would give me a little local anaesthetic, and I said what a shame they didn’t do that beforehand! I was told that the injection of the local would have been as painful as the cannula… Then a little antibiotic, and finally the anaesthetic.
I came round in the recovery ward, and my first conscious thought was, “Oh no… I forgot to set my alarm and I’ve overslept and missed my appointment!”
I was told that all had gone well. I felt very shaky and shivery for a while and was given oxygen through the mask I still had on, but this eventually passed once they got me back on Ricky Grant. I was given a nice cup of tea and allowed to recover for a while. The whole procedure took most of the morning, and I was given a Snack Pack with some delicious sandwiches for lunch, and more tea, and then the chemo began.
Because I’d had a surgical procedure, I was on the treatment couch for the whole time – it was a lot more comfortable than I would have been in a chair, and at the end I requested this for each treatment, especially as I often have a rest in the afternoon and with my M.E., being able to lie down more or less horizontally is a lot more comfortable and restful for me. They said that would be fine, as long as there was a spare couch – there may be others who have had a surgical procedure like me, or there may be emergency admissions of patients with chemotherapy-induced neutropenia (severe infection as a result of low levels of white blood cells).
When the port-a-cath was installed, Dr. Isaacs also inserted a gripper needle – the special hook-shaped needle used to access the port, shaped like this to anchor it securely, so it was all ready to go.
The first thing to be done was to flush out the port with saline, and a little negative pressure drew some blood back into the syringe, indicating that everything was functioning properly. After this I was given a dose of anti-emetic medication and a small dose of steroid – I said I’d prefer not to have steroids because they do tend to pile on the weight, but she said this was only a small dose, and I’d also be having only a minimal dose of dexamethasone orally at home, for a very limited period, and it would not have this effect. Its benefit is to help prevent nausea, to maintain appetite which can be diminished during chemotherapy, and also to give one a feeling of wellbeing to counteract the unpleasantness of the chemotherapy. I would also have some ondansetron (anti-emetic) orally for a couple of days at home.
Because saline is not compatible with oxaliplatin, the chemotherapy drug I am receiving, the latter is given in conjunction with glucose. Before beginning the chemotherapy, the port was again flushed, this time with glucose, and then the oxaliplatin was given – the bag contained approximately half a litre which surprised me – I had no idea I would be receiving so much, but of course it is in dilute form.
All these infusions take place through a single line into the port. The various bags on the drip trolley each have their own individual lines complete with a clamp to open and close them, and these connect into the single line, looking something like the branches of a tree. This is a very efficient system and enables them to change the substance being infused without interfering with the port or gripper needle at all, which is more comfortable for the patient, and reduces the risk of infection. It was quite hypnotic, watching the drip-drip-drip and seeing the level going down, and watching the countdown on the display. As it came to the end, I was reminded of the countdown on Ebay and you are on tenterhooks, wondering if you’ve won your bid, or whether someone will sneak in and beat you at the last second!
During the infusion I needed to go to the loo, which was an interesting experience. Because I needed to use my wheelchair which requires two hands, I had to have another hand to bring my IV pole (the machine operates in battery mode when unplugged from the wall). My hubby did this for me, and it was all I could do to make him walk slowly and keep an eye on where I was behind him so that he didn’t pull out the connections!! (He’s never been big on spatial awareness, I’m afraid…) If I were to go any faster I’d have been in danger of ramming the back of his legs! The disabled loo we used was plenty large enough for one person and a wheelchair, but it was distinctly cramped with two people, a wheelchair and an IV pole! Later my hubby did some recon and discovered a disabled loo of palatial proportions at the end of the corridor with room for all this, and the swinging of several felines besides. (NOT that I am in the habit of indulging in this latter practice, I hasten to add.)
The infusion was supposed to take four hours, but when the machine had finished its countdown there was still some oxaliplatin in the bag, so the machine was set up again, and twice more, until they were satisfied I’d had every last drop! They kept squeezing the contents down to the bottom of the bag, and I was reminded of the process of emptying my stoma bag. The whole process took about four and a half hours not counting the various flushings, and then the port was again flushed with glucose, and a final flush of Hepsal (heparin and saline) – the heparin acts as an anticoagulant to prevent blood clotting in the port or catheter. With a PICC line, this flushing has to take place every week, necessitating a visit from the district nurse or an appointment at one’s GP surgery, but the port-a-cath is low maintenance, being completely embedded under the skin, and only requiring flushing at each treatment, which was one of the reasons I was so keen to have it.
During the whole of the treatment I felt no ill effects. I was very tired and needed to rest – a combination of an early start and a long day, and the effects of the surgical procedure. I dozed for part of the time. My lovely hubby stayed with me throughout, despite my protestations that it really wasn’t necessary and that I was in good hands, but he felt better about staying, at least for this first time.
Forty-eight hours before each treatment I will need to have blood tests to check my blood count which is affected by the chemotherapy. Unfortunately the district nurse is not permitted to take bloods through the port, so I have to go back to the Ricky Grant Unit to have this done each time, so it’s another trip to the hospital for my poor hubby! He is being so good about it all.
Because the surgery had only just been done when the treatment began, there was some bleeding from the incision over the port, so when the treatment was finished, they removed the dressing (using some of the adhesive remover spray from my emergency stoma kit!) and a fresh, temporary dressing applied. I have to go back tomorrow morning for this to be removed, the wound checked and cleaned, and a new dressing applied. The small incision at the base of my neck is fine and doesn’t need touching. They will also flush the port at the same time.
When I was first checked in at Ricky Grant, the anaesthetist came to see me, and gave me a very nice little pack to accompany the port-a-cath.

It was fastened closed with a Velcro dot, and included a checklist, an identification card, a user manual and a wrist band.

The checklist and card.

The card has my basic details on the back. I have to keep it with me at all times, and present it to any clinician who is to perform any venous procedure (taking blood, the injection of contrast medium for scans, etc.). They also gave one to my hubby.
The user manual, containing details of the port and its installation, how it is used, and the risks associated with it.

A nice touch was the cool wrist band also included – gorgeous colour, and I love the gradation of light to dark! As well as being a great fashion accessory, it also serves to alert the emergency teams should I be involved in an accident.

After being given the “Udderly sMOOth” moisturising cream at my New Patient Talk appointment, I ordered some white cotton gloves and socks to wear at night, to enable the moisturiser to work efficiently and without making my bedding or clothing greasy. I got these on Amazon and they were very cheap.


Having been warned about the problems with peripheral neuropathy, I did some online research to see if there was anything I could do to minimise this unpleasant side-effect, and found these gloves with silver incorporated into their fabric. Their primary use is for Reynaud’s and scleroderma but also listed is chemotherapy-induced peripheral neuropathy, and there were plenty of positive reviews, so I ordered some.


(Lump is the dressing where the cannula was.) I am pleased to say that all these products had arrived by the time I got home this evening, because by the time I went upstairs to the bathroom prior to eating, the neuropathy had begun – I tried laying my hand on the cold tiles of my bathroom counter and immediately withdrew my hand as it felt as if it had been electrocuted!! A sharp, buzzing pain. Very unpleasant. Not what I had expected – I thought I might get a little tingling and numbness!
I put the silver gloves on straight away and have been wearing them all evening. They are a soft fine knit and very comfortable, and I have not yet encountered any activity that they prevent me from doing, including operating the computer. My hands do feel warm, but not excessively so, and they are certainly not sweating. I am highly delighted with the gloves and feel confident that I can touch what I like now with no ill effects. I shall take them in to the Ricky Grant Unit and show the staff, because their other patients might be very glad to know they are available, as this is a very common side effect – so much so that it is really to be expected with oxaliplatin.
I bought two pairs of each of all these products so I can have one on, one in the wash. They should see me through the duration of the treatment.
When I started to eat my supper, the first mouthful caused an unpleasant painful sensation as if my salivary glands were inflamed – I remember this feeling as a child when I had mumps – but when I ate some more the feeling had gone. Dr. Lo, the oncologist, warned me of this side effect which is a spasm of the jaw. What I experienced was obviously a mild form of this, and as I accumulate more of the drug in my system, I think I can expect this to become worse. I am not very happy about this because it was listed as a “possible” side effect that most people do not get.
So, my first cycle is complete. One down, about 10 more to go!! Each one I have done is one less to do, but I am aware that with the effects of the drug being cumulative over time, I am likely to feel increasingly unwell as time goes on. At least the first one was not too bad at all, and I have taken steps to deal with the unpleasant side effects, and I have the ondansetron and dexamethasone tablets to take to counteract any feelings of nausea in the first couple of days after each cycle. I was also given some domperidrone as an adjunct for this symptom should it persist – I can take these as and when I need them, three times a day, but the nurse explained that many people never need to take them. I was also prescribed some paracetamol to relieve the post-operative pain around the port-a-cath. They are certainly looking after me!
My next cycle will be on Friday 12th June, also at 12.30 p.m.
Saturday 23rd May 2015
Port Dressing Changed
We went back to the Ricky Grant Unit this morning to have the dressing over the port-a-cath wound changed. It bled a bit during the treatment yesterday and they put on a temporary dressing.
This is how it looks now.


The top picture shows both wounds. The top wound is where the catheter was inserted into the internal jugular vein and threaded down into the superior vena cava, the main vein which enters the right atrium of the heart. The bottom, larger wound (also illustrated below) is where the pocket was created for the insertion of the port itself, which rests against the chest wall. There is only a small lump to indicate where the port is, just above the wound. Dr. Isaacs created a tunnel between the two, and under X-ray guidance, pulled the other end of the catheter through this and connected it to the port. It is all healing nicely, and the scars should be virtually invisible eventually.
I was given a tiny tube of Ametop (tetracaine), a local anaesthetic gel, which has to be kept in the fridge.

Half an hour before my next treatment I have to squeeze the whole of the contents into a mound onto the top of the port and cover it with a clear dressing which she also provided, without rubbing it in, and it will soak into the skin and numb it, ready for the insertion of the gripper needle. The effects should last several hours. Over time, scar tissue will develop over the site, rendering it less sensitive, and the Ametop may no longer be needed for future treatments.
I wish they had applied some of this to my hand before inserting the cannula just before I had my anaesthetic on Friday!
I told them about the silver gloves and the nurse was very interested, and made a note of the website, and said she would tell the rest of the team. I said that since peripheral neuropathy is such a common side-effect of oxaliplatin, we ought to be able to get these gloves on prescription! They are fairly pricey but so far I have not regretted a single penny! They are brilliant.
All day I was feeling pretty good. OK, the peripheral neuropathy was bad and I had to keep the gloves on, and I got the awful jaw sensation when I started eating, but apart from that, no real problems. I do not expect to continue to feel this good with subsequent treatments because the effects are cumulative.
Sunday 24th May 2015
Not Feeling Too Good Today
When I woke this morning I felt slightly nauseous and this hadn’t improved by lunch time. I decided to look online for a ginger smoothie recipe and came up with this:
I substituted 2 dates for the honey as I have been told to keep off honey in case of infection. I used green tea – I made up a bottle of this the other day which I keep in the fridge, and simply heated some up to make this a nice warm drink. I also used cocoa powder instead of cacao as I don’t yet have any of the latter – cacao is better because it is produced by cold-pressing the cocoa beans, whereas cocoa is cacao that has been heated to a high temperature, thus losing some of the goodness. Cacao is now on my list of ingredients to get! This elixir (like a smoothie but slightly more liquid) contains ginger which is good for nausea and it also said it was immune boosting, and it certainly contains some good stuff! It was also delicious.
My hubby did manage to persuade me to eat a small portion of lunch and then I went to sleep for a while – feeling really wiped out.
I was delighted when I got up this morning, to discover that the peripheral neuropathy had disappeared, but when I started to make my smoothie it came back again, so I’ve got the gloves on again. I also noticed a slight diminution in fine motor skills, making typing difficult, but this has improved.
I am a bit disappointed to feel so rough today because I felt really good yesterday and thought after the first treatment that it wouldn’t be so bad after all. My hubby said he’d had a word with the nurse yesterday and she said I might not feel so hot on Day 3 – I suppose it’s all starting to filter through my system now. I think the fatigue is probably a result of one’s body trying to respond to the damage and destruction caused to normal tissue by the chemo – one always feels exhausted during an infection or after injury or surgery as the body’s energy is expended in the work of repair. I am hoping to feel better tomorrow, and to notice some improvement during the next week to ten days. It would nice to be feeling well again before my next treatment.
Thursday 28th May 2015
Follow-Up Appointment with Surgeon
This morning I had my follow-up appointment with Mr. Pullan, the surgeon who performed my operation to remove my large bowel and create the ileostomy. He is pleased with how everything has gone. I asked him about my rectal stump which he says is very short. I wanted to know if it was normal to be continuing to produce such large quantities of mucus from it – it is not every day but every two or three days I keep feeling the need to poo, and can feel it come away into the loo. He said it was quite normal, and it could take months to clear up completely, and that this process would be hindered by the chemo. It’s not a major problem for me – more of a slight irritation, but I am reassured that all is normal, and there isn’t anything going on that I should worry about.
He said he and Dr. Lo, the oncologist, would be “leapfrogging” as far as my future appointments were concerned – they would be consulting regularly about me and how I was getting on, and keeping an eye on me between them. Over the coming months and years I shall have a series of CT scans to make sure that the cancer has not returned anywhere else in my body.
We discussed the effects of the chemo a little, and he commiserated with me over this, and said how good Dr. Lo was at assessing statistics and the pros and cons of having chemo after surgery to remove a cancer like mine. I agreed that it was a good thing and that it would give me the best chance of getting over this completely in the long run, however unpleasant it might be for the next six months.
Although the side effects from the chemo have diminished somewhat as the week has gone on, I am feeling far from well. The episodes of nausea have gone, but the peripheral neuropathy is still lurking around, causing me to be careful when handling cold things – preparing some strawberries straight from the fridge tonight set it off, but touching normally cold things like my bathroom tiles or metal door handles is not setting it off now. Food tends to be pretty tasteless and my appetite is poor. The worst part is feeling totally wiped out and needing lots of rest and sleep during the day and this makes me feel very unwell. I am not sleeping well because Kermit, my stoma, is being affected by the chemo and producing a lot more output, which is runny and gassy, and last night I was up twice during the night emptying the bag. I was told this would happen and I am taking loperamide (Immodium) and eating marshmallows to try and thicken things up a bit, and taking rehydration drinks.
I had an appointment with the stoma nurse this morning too, and I will be updating my Gutless Bag Lady blog with details of that.
Over the bank holiday weekend my stairlift broke down (some timing!) and I have been having problems dealing with the company who are so unbusinesslike and unreliable! I am trapped, because only they can repair it – none of the local firms will touch it – and they keep promising things they don’t follow through on, and they keep passing me from pillar to post, saying I shouldn’t have phoned this number and I need that number, then to be told that that number is wrong! They promised to come out on Tuesday but when nobody came by 3 p.m. I phoned again and they said “Who told you someone would come today?” They then informed me they couldn’t come till Friday! The man had the gall to say that because the problem was intermittent, it was not deemed urgent! I said that as far as I was concerned, the stairlift was not working if it was not reliable – I can’t get stuck half way, so I can’t use it! The stairs are bad enough with my normal M.E., but with chemo exhaustion overlaid on top, they have turned into Mt. Everest. I am keeping my emergency stoma kit downstairs so at least I can empty the bag in the downstairs loo, and not have to keep going up to do it, and I am restricting the number of times I have to use the stairs as much as possible. The downstairs loo is inconvenient because it is small and narrow, with no basin, and the pan itself is smaller, giving little room for bag emptying. To change the bag I have to use my bathroom where all my kit is, and where I’ve got the basin and plenty of room to lay things out. However, I only have to change the bag every three days as it is drainable.
I am not sure whether this is a side effect of the chemo, but over the past couple of days I’ve felt quite down emotionally, and a bit weepy and vulnerable. It may just be everything I’ve been through recently (and the problems with the stairlift), and general exhaustion, and also the thought of this going on for the next six months, now I’ve had a taste of just how poorly the treatment can make one feel.
Comments from my old blog
glitterandglue
24 May 2015 at 21:52
Not sure what happens when I try to come and leave a comment on your site – but it always disappears. Usually have to re-type. Getting cunning – copy and paste is now being tried… Wow, Shoshi, what I lot I have had to read to catch up. Take care of yourselves, both of you, now your cycles of treatment have started. You obviously have a great team at the centre, and at the hospital. That’s SO encouraging for you. Wishing you every blessing, and continuing to pray for you both. Much love to you. Margaret
Anne
29 May 2015 at 01:39
Hello Shoshi – I have been catching up with all your news! A lot to catch up with. Please don’t think I’d forgotten you. I think of you often and you are in my prayers each evening. I have had a very busy month of May and indeed have not been at home much. Visiting my son, mum and then on to Cornwall for a much needed break and back and up to Yorkshire again to visit our son and babysit. I need to catch up with my blog at some point. Photos will be tricky as our camera has decided to ‘ give up’. Your treatment sounds dreadful but as you say the alternative is far worse! It was good to read you had been crafting again and I like your cards. Also good that you got to see your friend to celebrate her 80th birthday. Well I need go try and sleep it’s 1.36 am and I have an appointment in morning at the doctor’s ! Only routine. Hang in there! Gentle hugs Anne x